WHO warns against use of Kenya-tested Ebola virus vaccine in current outbreak
Experts say Ervebo vaccine tested should only be used in controlled trials, not mass vaccination.
by JOHN MUCHANGI
Audio By Vocalize
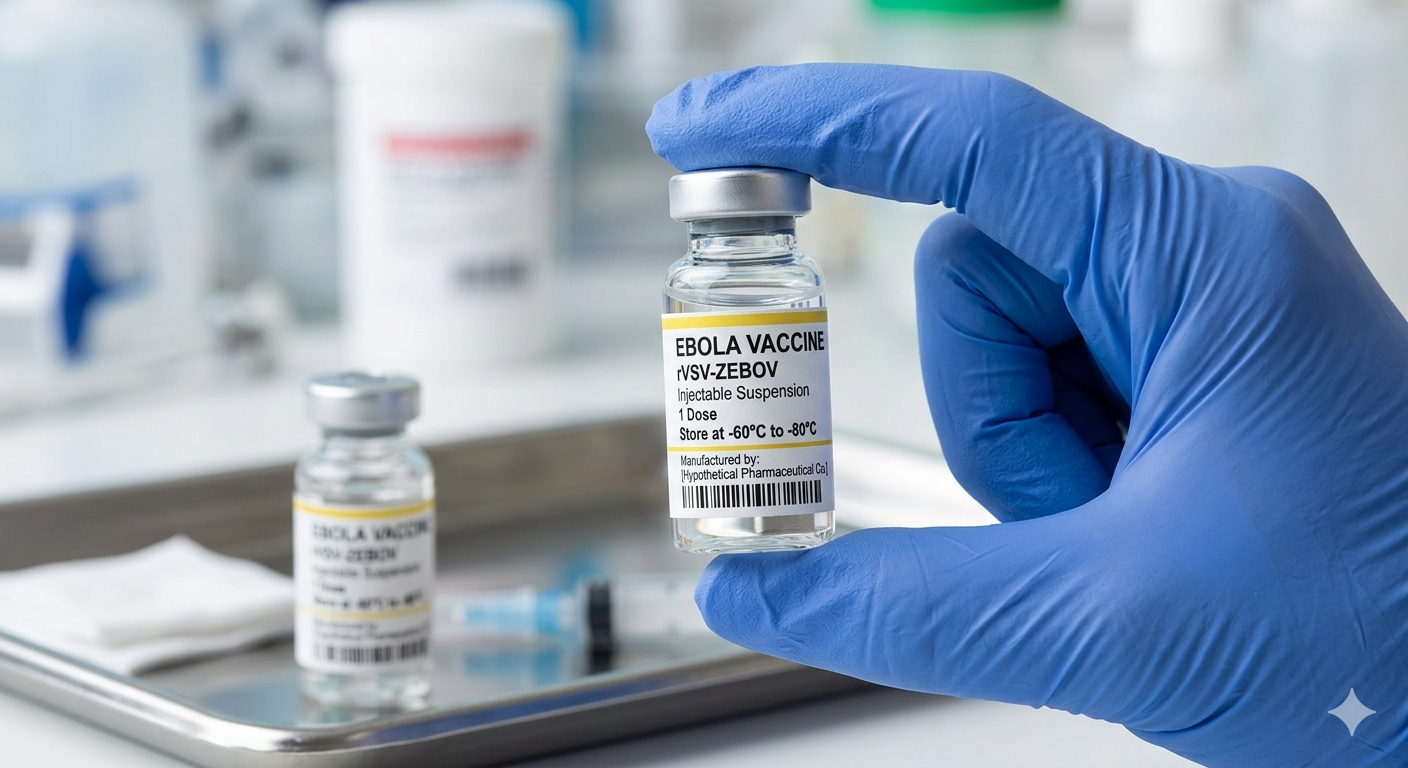
The World Health Organization has said the world's only licensed Ebola vaccine, which was partly tested in Kenya nearly 10 years
ago, should not be used to widely vaccinate people in the current outbreak.
The WHO said the Ervebo vaccine can only be used in carefully controlled clinical trials.
The vaccine, which is used to protect against Ebola caused by the Zaire strain,
was partly tested in Kenya from 2016, where about 40 healthy adult volunteers
took part in early safety studies in Kilifi county.
Those trials were designed to check whether the vaccine is safe and whether
it can stimulate an immune response in the body, not whether it prevents
disease during outbreaks.
WHO said the vaccine should not be assumed to work against a different Ebola
type known as the Bundibugyo virus, which is driving current outbreaks in the
Democratic Republic of the Congo and Uganda.
Bundibugyo virus disease is caused by a different species of the Ebola virus
from the Zaire strain that Ervebo targets. Scientists said this difference is
important because vaccines are often designed to match a specific virus type,
and protection against one strain does not always extend to another.
“Ervebo is not licensed for prevention of
BVD and evidence on cross-protection to other Ebola virus species remains
limited and inconclusive. WHO recommends that Ervebo should not be used outside
carefully designed research settings, to allow for its performance against BDV
to be assessed.”
The global health agency added that all Ebola vaccines and treatments
identified for the current outbreak must only be used within clinical trials.
“The WHO advisory groups recommended that all the products identified and
considered be used exclusively within clinical trials to generate robust data
and ensure safe, ethical, and effective research,” WHO said.
The guidance follows meetings convened by WHO with its R&D Blueprint
technical advisory groups, the Strategic Advisory Group of Experts on
Immunization (SAGE), and its Ebola vaccine working group. The experts were
reviewing possible vaccines and treatments for Bundibugyo virus disease, which
currently has no approved vaccine or cure.
WHO said the goal is to ensure that any use of experimental products
generates strong scientific evidence while protecting patients and communities.
For treatment, WHO experts recommended three candidate medicines for
evaluation in clinical trials among confirmed cases. These are monoclonal antibodies
MBP134 and Maftivimab, and the antiviral drug remdesivir. Experts also
suggested studying combination therapy using a monoclonal antibody together
with remdesivir.
For prevention, the oral antiviral obeldesivir was identified as a priority
candidate for post-exposure use among contacts of infected patients. However,
WHO warned that this approach depends on effective contact tracing, which can
be difficult in outbreak areas.
On vaccines, WHO identified the single-dose rVSV Bundibugyo vaccine,
developed by the International AIDS Vaccine Initiative (IAVI), as one of the
most promising candidates. However, it is expected to take 7–9 months before it
is ready for full clinical trial evaluation.
Another candidate vaccine, ChAdOx1 Bundibugyo, developed by Oxford
University and the Serum Institute of India, could be ready in two to three months
for clinical trials, though WHO said more animal data is still required before
it can be fully prioritised.
Experts also discussed how different vaccine strategies may be used
depending on risk levels. A single-dose vaccine may be used for contacts of
confirmed cases, while a two-dose approach could be considered for high-risk
groups such as health workers and emergency responders.
Despite Ervebo’s approval for Ebola Zaire, WHO stressed that its
effectiveness against Bundibugyo virus remains uncertain and cannot be assumed.
The vaccine “is not licensed for prevention of BVD and evidence on
cross-protection to other Ebola virus species remains limited and
inconclusive,” WHO said.
WHO also said Ervebo should only be used in research settings when assessing
whether it offers any protection against the Bundibugyo strain.
The agency is now working with governments in the DRC and Uganda, the Africa
Centres for Disease Control and Prevention (Africa CDC), and other partners to
support the design of clinical trials in outbreak areas.
At the same time, WHO warned that vaccines and experimental treatments must
not distract from basic outbreak control measures. These include surveillance,
rapid testing, isolation of patients, contact tracing, infection prevention in
hospitals, and safe and dignified burials.
“In the meantime, our priority is to stop transmission with tools that we
have used for decades of Ebola responses, which include disease surveillance,
rapid testing and diagnosis, contact tracing, isolation and care for patients,
infection prevention and control, community engagement, and safe and dignified
burials,” WHO said.
The organisation called for faster access to essential supplies, stronger
community trust, and coordinated investment in Ebola research.
This is premium content
Subscribe to Continue Reading
Help us continue bringing you unbiased news, in-depth investigations, and diverse perspectives. Your subscription keeps our mission alive and empowers us to provide high-quality, trustworthy journalism. Join us today to make a difference!






![[PHOTOS] The new Ngong –Naivasha Road viaduct](https://cdn.radioafrica.digital/image/2026/06/64d4f771-4432-4aee-ba3c-2f304c4436ec.jpg)










![[PHOTOS] 'Mr Speaker Sir' Gen Z protester in court](https://cdn.radioafrica.digital/image/2026/06/b3e62d8e-25c3-4780-90f9-4eb48b1ce8a7.jpg)
