 Sumantha Chaudhary, adviser of Mumbai-based
Pharmexcil, and director Rollins John during a presentation at the agency’s
offices in Mumbai on June 9, 2025/ Eliud Kibii.
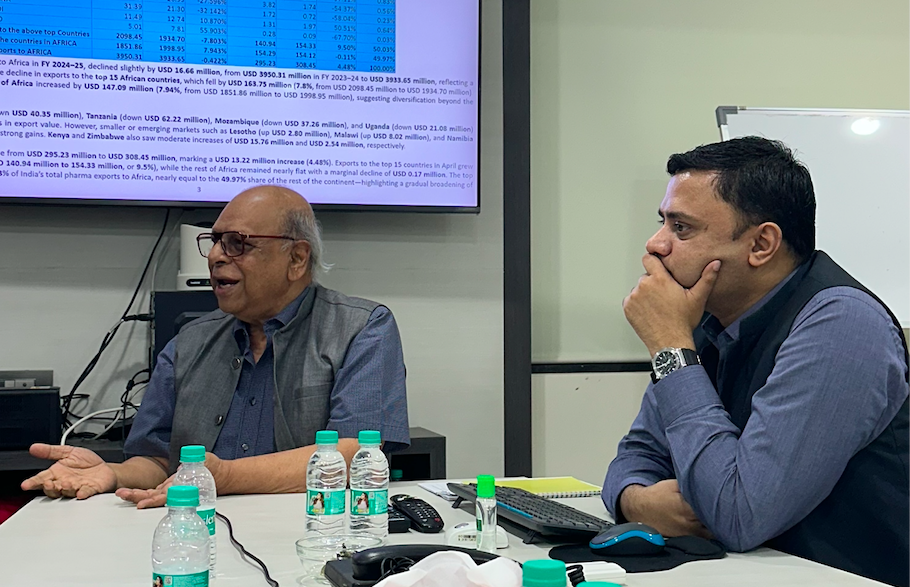
Sumantha Chaudhary, adviser of Mumbai-based
Pharmexcil, and director Rollins John during a presentation at the agency’s
offices in Mumbai on June 9, 2025/ Eliud Kibii.
Kenyans just like other Africans will continue to dig deeper into their pockets to buy drugs imported from India due to unfavorable business regimes.
According to officials of India’s Pharmaceutical Export Promotion Council (Pharmexil), Indian firms are forced to incur additional costs such as recurrent approval and inspection costs, promotion and marketing expenses and transport costs.
Further, due to delayed registration and lack of regulatory harmonization, countries in Africa are not getting the latest drugs, and by the time the products get to the market, prices have already changed.
Sumantha Chaudhary, the adviser of the Mumbai-based Pharmexcil, said it takes between four to five years for Indian companies to get approvals and get drugs to the continent, which means availability of such medicine and vaccinations is limited.
“If then it takes that long, it means it will come at a higher price. Treatment becomes too expensive, and you will be surprised that some patients find it cheaper to travel to India for treatment”, Chaudhary told journalists from East and Southern Africa in Mumbai Monday.
Chaudhary added
that lack of harmonized and coordinated platforms for African states to import
drugs and vaccines was also a bottleneck.
“For instance, the EAC had indicated it would jointly recognize approval of drugs for supply across the community but this is yet to happen. This means it takes more time dealing with each state separately. Institutions mandated with regulation in Africa need to find a way of streamlining the approval processes,” he said.
In this regard, they noted that the disjointed small markets and the weak intra-African trade — despite AFCTA — have been among the contributing factors to the challenge of supplying to Africa, as well as even establishing manufacturing bases on the continent.
“Take for example you are manufacturing a syrup in Nairobi. You would still need to get almost all the materials, including bottles, from here [India] because they are not available there. This means it will end up being very expensive, a cost that is passed on to the product.
“And while they can be trained, you will still need to have adequate technicians for manufacturing,” he added.
Rollins John, a director at Pharmexcil added that there is need to incentivize investors by having coordinated regional agreements that would allow a firm establishing in one country and able to supply across the region.
“If we set up in Kenya, and can only sell within the country, that will not be sufficient for survival. That company must be able to sell across the neigbouring countries for commercial viability.
“Unfortunately, the intra-country relationship is not so strong to allow this arrangement to happen,” John said.
Pharmexcil is a state agency mandated with the promotion of pharmaceutical exports from India.
It was set up under Foreign Trade Policy by the Ministry of Commerce and Industry in May 2004 to facilitate exports of Indian pharmaceuticals and allied products. These include bulk drugs, formulations, biotech products, Indian systems of medicines, herbal products and diagnostics, as well as clinical research.
India’s pharmaceutical exports to Africa have exhibited a strong upward trend over the past two decades, rising steadily from $75 million in 2007 to nearly $3.93 billion in 2025, a more than fivefold increase.
Kenya was the third top destination for Indian pharmaceuticals in 2024-2025 after South Africa and Nigeria.
“South Africa remained the top destination despite a 5.62% year-on-year fall, followed by Nigeria and Kenya, which showed moderate growth of 5.36% and 3.71% respectively … Countries like Zimbabwe (91.55%), Kenya (48.29%), and Nigeria (45.17%) witnessed sharp increases, indicating a rebound in demand,” Pharmexcil data says.